
Why Zambia is Rethinking Tuberculosis Testing, and Why Validation Must Come First

Inside a small laboratory at the University Teaching Hospital in Lusaka, the capital of Zambia, a technician splits a sputum sample in two. Half goes into a GeneXpert machine, the workhorse of tuberculosis (TB) diagnosis in Zambia. The other half goes into a near-point-of-care molecular device, small enough to sit beside a phone, powered by battery or external power, and capable of delivering results in under an hour.
The technician is comparing the new test’s result with the country’s established molecular testing platform. Before any new diagnostic tool can be used in Zambia, it must prove itself against the machines the country already trusts. “Each country is supposed to validate it,” said Dr Eddie Somuneti Solo, Head of the Tuberculosis Laboratory at the University Teaching Hospital, running the comparison. “Because the device may have been built and tested far from where it is now being deployed,” he explained, “local validation isn’t optional. Those requirements say you need to validate it and see the results.”

However, what is being tested is not just the device; it is a question Zambia has been circling for years and was finally forced to answer in 2025. What happens to a TB programme built around expensive, power-heavy machines when the external funding that keeps them running is suddenly interrupted?
Zambia is among the world’s 30 high-burdencountries for TB. An estimated58,000 people develop TB disease each year, killing between 5,000 and 8,000, a toll that may be underestimated when undiagnosed TB is recorded under broader respiratory causes of death.
On official cause-of-death statistics, TB sits well down the list, behind non-communicable diseases (NCDs) and a broader category titled “respiratory infections.” Dr Angel Mubanga, Zambia’s National TB and Leprosy Programme Coordinator at the Ministry of Health, believes that “many of those respiratory deaths are TB that was never caught in time,” he argued, “and the picture changes completely.”
Yet once TB is diagnosed, Zambia’s treatment outcomes are comparatively strong. The treatment success rate has stayed above 90% for years, ahead of the World Health Organization (WHO) benchmark for high-burden countries, suggesting that the disease’s grip on Zambia has never really been a treatment problem, it has been a diagnosis problem.
Motorbikes, microscopes, and a courier system stretched thin
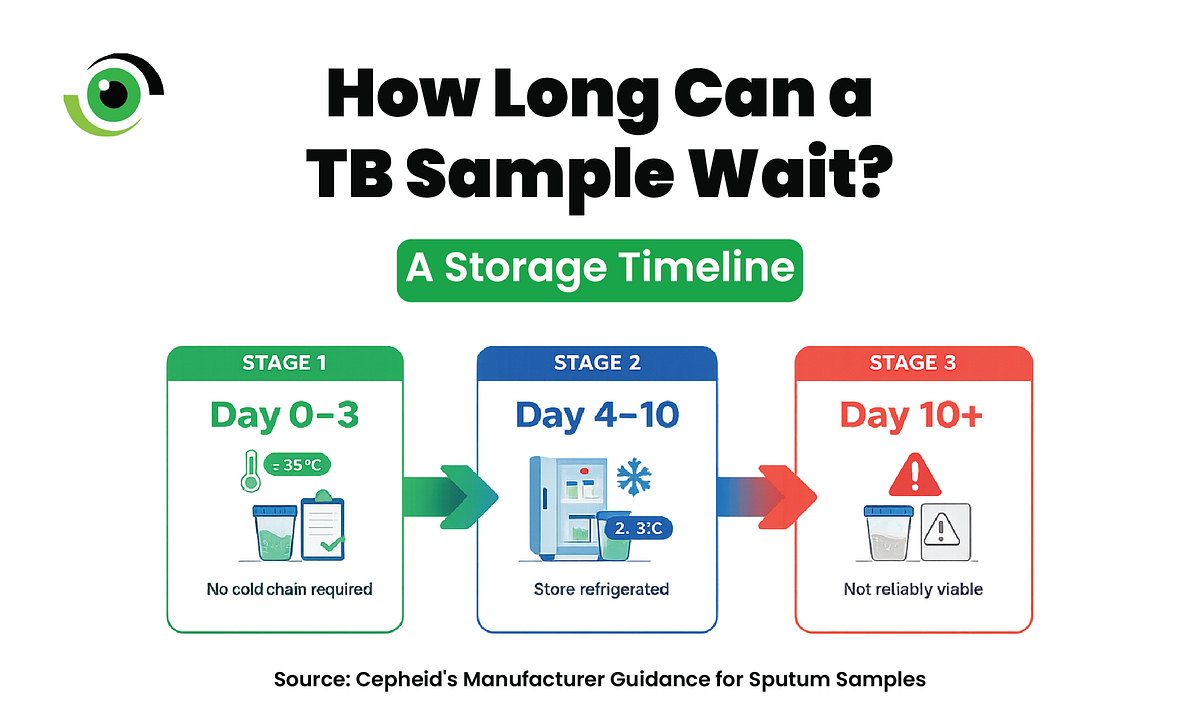
The country hasmore than 4,000 health facilities spread across 116 districts, many of them hours apart by road. As of 2024, only about 33% of those facilities could test for TB. This meant that the sputum sample had to be transported by motorbike riders, carried in cooler boxes with ice, to keep it viable for clinics and laboratories with GeneXpert or Truenatmachines, thereby adding time, cost, and risk of sample loss.
The system’s other weakness was the testing machines themselves. GeneXpert needs stable power and an air-conditioned room. In 2020, drought reduced hydropower output, leading to nationwide load shedding. Machines that depended on a stable power supply could not run continuously for hours. Samples accumulated faster than laboratories could process them, and some were no longer viable by the time they could be processed. That same year, Zambia recorded its highest number of presumptive TB cases but its lowest diagnostic yield.
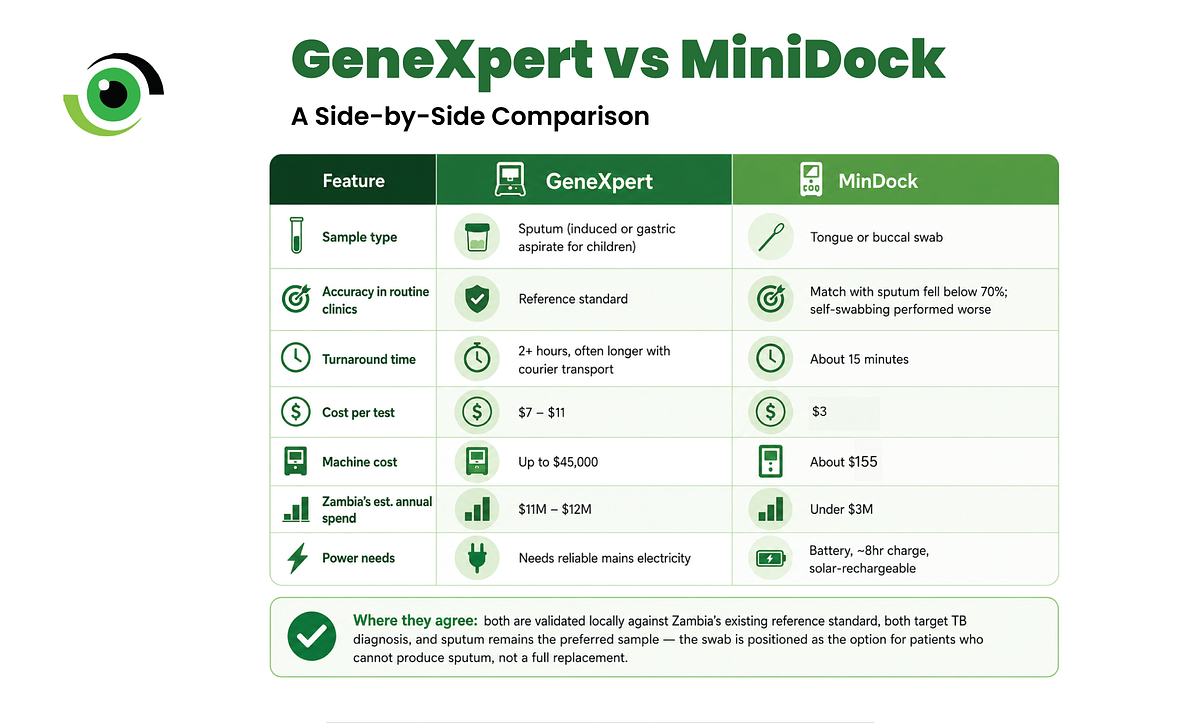
In 2025, the USAID funding that paid for most of Zambia’s GeneXpert cartridges, without which the machines cannot run a single test, costing $7 to $11 each, was suspended without warning. “No one expected to see the thing that happened, would happen,” Dr Mubanga said. “It just happened.” For six months, the country’s testing machines ran on whatever cartridges the government could fund on its own.
The diagnostic device meant to make a difference
On March 24, 2026, the WHO recommended a new tool that is compact, battery-powered molecular tests known as a near-point-of-care device, designed to work close to where patients actually are, rather than in a centralised lab.
Zambia’s national reference laboratory began validating the MiniDock device manufactured by Pluslife, a Chinese diagnostics company. The rollout is part of a Global Fund-led Early Adopter initiative, and led by the Global Fund to Fight AIDS, Tuberculosis and Malaria.
The initiative aims to improve early detection and expand access to quality TB diagnosis, supported by the Children’s Investment Fund Foundation(CIFF) and implemented on the ground by the Aurum Institute, and will deliver nearly 3 million fast, accurate TB tests across 13 countries to people and places that have never had access before.
The MiniDock uses a tongue swab and, in some protocols, other oral swab approaches, which seems like a breakthrough for a disease where getting a usable sputum sample, especially from children, is often described by health workers and caregivers as messy.
Redesigning the courier system, not retiring it
Currently, Zambia’s strategy retains GeneXpert in the diagnostic pathway but shifts its role to a confirmatory test, used only for the small proportion of samples that test positive from the MiniDock. This is to rule out the chances of a false positive and to detect resistance to rifampicin, one of the most important first-line TB drugs. In practice, only about 4 to 12 out of every 100 people tested require confirmation.
Under the new model, the courier riders who once carried every sample to a hub lab would only need to carry that smaller fraction. “Riders would not disappear,” Dr Solo said. “They would simply be needed less frequently.”
So far, however, the devices had not yet been used for routine patient testing in Zambia. The country has secured 134 units through the Global Fund’s early-adopter programme, alongside smaller batches procured by local research partners. These devices will be deployed in an initial 45 to 60 facilities chosen for their high testing volumes rather than through a nationwide rollout.
The first entry point under consideration is health posts, the lowest tier of the health system that still has a nurse on staff. The phased approach is deliberate, echoing the rollout of HIV self-testing, which was introduced to lay counsellors only after years of evidence had established its safety and effectiveness.
The TB programme intends to follow a similar path: first, validate the technology with trained health workers, then consider whether it can be used safely at the community level.
The gap between lab results and real-world clinical conditions means Zambia will need to continue testing the device as it rolls out more widely. The government will also need to fund this platform itself, instead of relying on outside donors to sustain it. But the real test is whether the programme can reach community health workers, the people who could bring testing and treatment directly to where Zambians live.
Zambia is not yet able to say that a battery-powered device will fix its TB response; what it can say is that, faced with a funding collapse it never saw coming and a climate it cannot control, it chose to test its way toward something less fragile, rather than wait for the next shock to make the decision for it.
Leave a Comment
Your email address will not be published. Required fields are marked *
Related Stories




