
From Autonomy to Accountability: Can Local Governments Deliver Better Primary Health Care in Nigeria?

About 70%of Nigerians depend on primary health care (PHC) centres for healthcare. For most people, this centre is the most frequent point of contact with any government service. The local government chairman is supposed to run it, fund it, and is responsible when it fails.
The Supreme Court’s July 2024 ruling confirmed that state governments had been unconstitutionally withholding council allocations for decades. Health financing data shows those allocations are the primary lever councils have for funding primary care. A national dialogue was convened in Abuja in June 2026 by the Association of Local Governments of Nigeria (ALGON) with support from the World Bank.
A ruling that promised more than it has delivered
In July 2024, Nigeria’s Supreme Court ordered that monthly statutory allocations to the country’s 774 local governments be paid directly from the federation account into each council’s dedicated account, ending decades in which councils received their funds through state-controlled joint accounts. President Tinubu welcomed the verdict, saying council leaders would now have to answer for whether services on the ground actually improved.
Nearly two years later, that promise is still mostly on paper. Between July 2024 and December 2025, state governments retained more than N7.43 trillion intended for local councils, channelling it through the very joint-account structure the court had already ruled unconstitutional.
For a council chairman trying to fix a leaking primary health centre roof or pay a community health worker on time, an autonomy that exists in a judgment cannot repair the roof, pay the worker, or restock the facility. They need the money sitting in their accounts, and for many councils, it still is not there.
The law already grants local governments that power. What remains unresolved is whether it ever reaches an account a chairman can spend from.
How BHCPF is meant to support frontline care
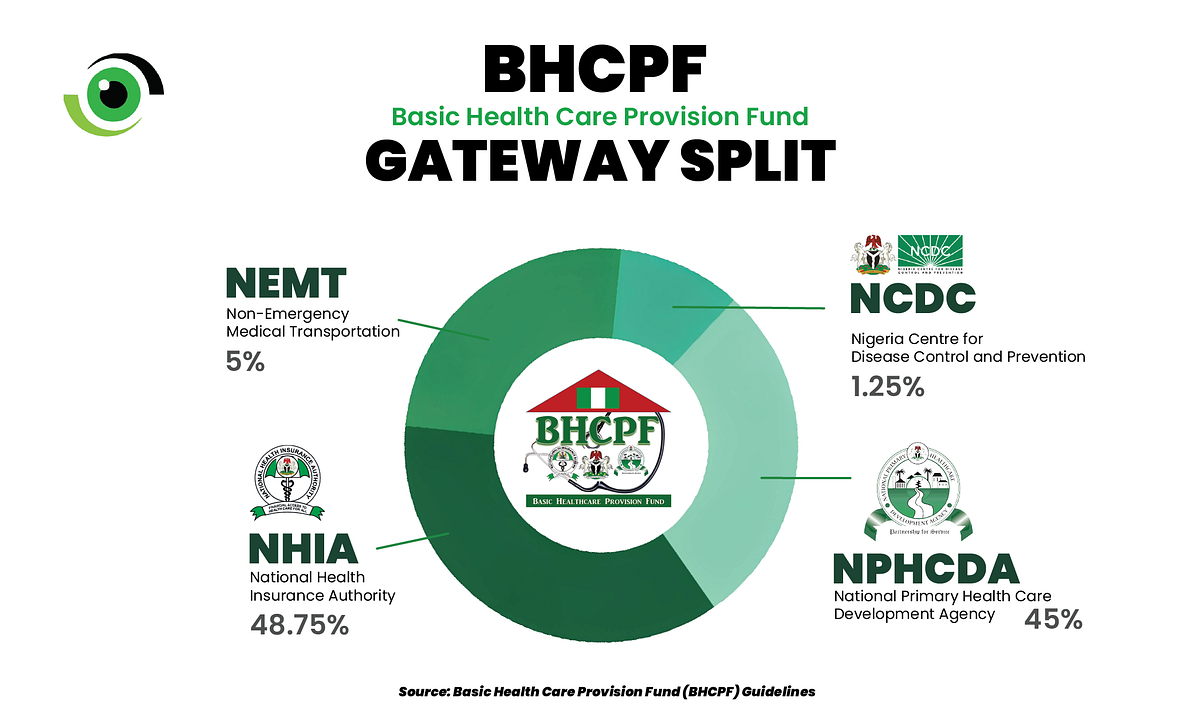
Where local government funds reach the front line, they are disbursed through the Basic Health Care Provision Fund (BHCPF), which is at present funded by at least 1 per cent of the Federal Government’s Consolidated Revenue Fund, and allocated across four gateways;
- 48.75% goes through the National Health Insurance Authority (NHIA) for insurance cover.
- 45% goes to facility-level needs such as drugs, equipment and community health worker pay through the National Primary Health Care Development Agency (NPHCDA).
- 5% supports emergency medical transport through the National Emergency Medical Treatment Committee (NEMTC).
- 1.25% funds outbreak preparedness through the Nigeria Centre for Disease Control and Prevention (NCDC).
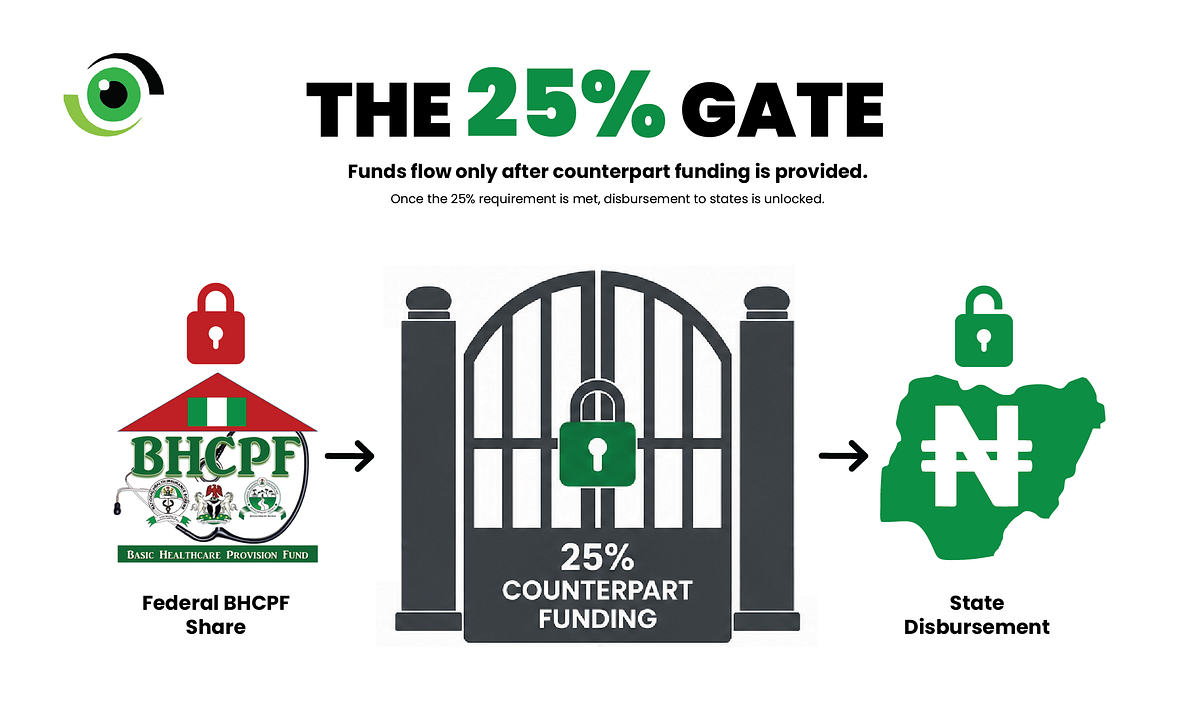
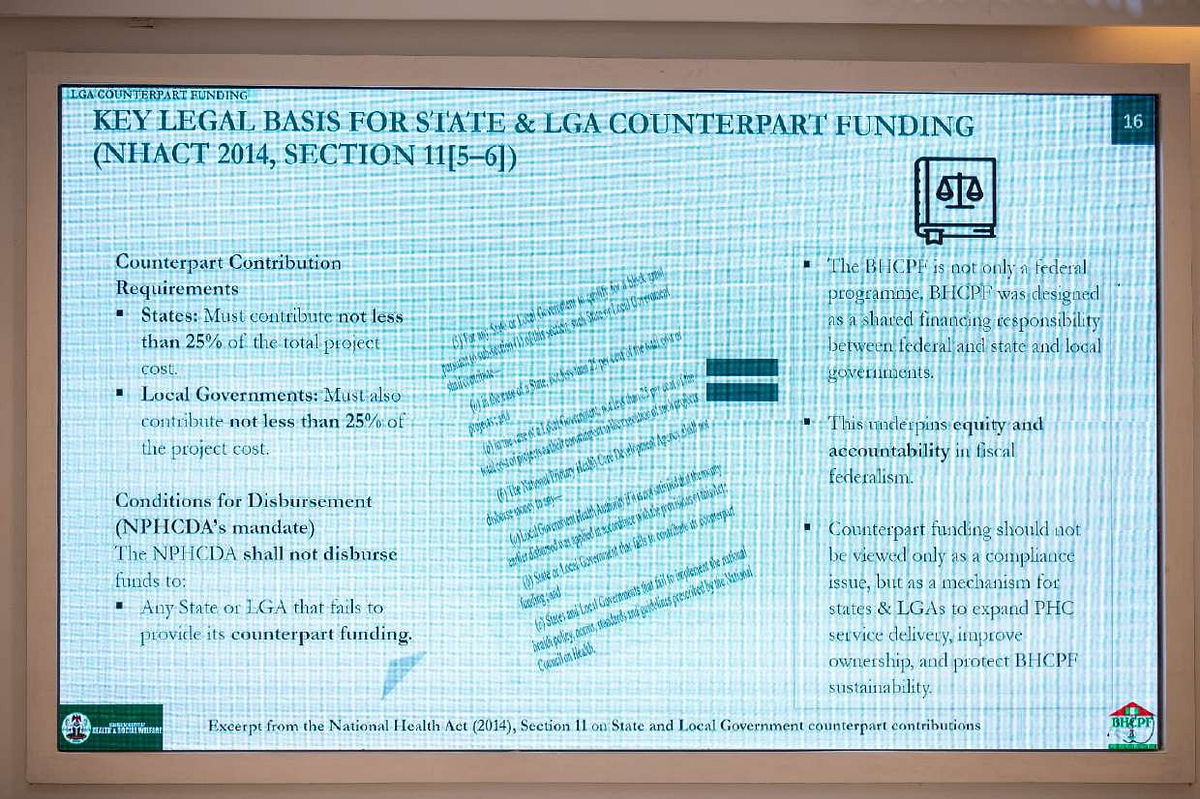
During a presentation on ‘Implementing Basic Healthcare Provision Fund (BHCPF) — Role of LGAs’ by Uzoma Nwankwo, the Director of the Basic Health Care Provision Fund (BHCPF) Secretariat, at the national dialogue, he highlighted that under the National Health Act (NHACT 2014, SECTION 11[5–6]), state governments must each contribute 25% of the project cost before the Federal Government transfers the BHCPF into the Treasury Single Accounts (TSAs) of the respective gateways.
No counterpart contribution, no disbursement. The structure is designed to enforce a direct link between what a council commits locally and what flows back to its facilities. A Local Government Health Authority that fails to mobilise its own 25% effectively locks its community out of a fund built to serve it. Autonomy, read this way, is less a gift than a test of whether a council shows up to claim what it’s owed.
What the data suggests
The national dialogue provided the clearest picture yet of how this counterpart funding requirement is shaping implementation. The Maternal and Neonatal Mortality Reduction Innovation Initiative (MAMII) tracking data, presented by Dr Dayo Adeyanju, the National Lead and Coordinator of MAMII, showed that across local government areas prioritised under the MAMII states, the share with at least one fully functioning emergency obstetric facility rose from 76% in October 2025 to 91% by May 2026. Antenatal care attendance in those same areas climbed from roughly 1.3 million pregnant women in 2023 to more than 2.1 million by 2025.
Community-based health worker coverage increased much more slowly, from 12% to 27% over that same seven-month stretch. This means that while more than 9 in 10 facilities are now functional, fewer than 3 in 10 communities are covered by community-based health workers.
Similarly, of the 172 priority local governments assessed nationally, only seven, just over 4.1%, had all four basic components of safe maternal care in place at once: at least one functional Basic Emergency Obstetric and Newborn Care (BEmONC) facility, at least one Comprehensive Emergency Obstetric and Newborn Care (CEmONC) facility, adequate Community-Based Health Worker (CHW) coverage, and operational Emergency Transport Services (ETS).

A delivery room with solar power and a functioning theatre is not the same thing as a delivery room with a trained health worker standing in it, and right now, Nigeria is building health infrastructure far faster than it is recruiting the health workers needed to staff it.
What local government leaders were asked to do
Throughout the day’s sessions, participants became increasingly specific about what they wanted local governments and other stakeholders to do. The World Bank’s presentation on broadening health insurance coverage at the ALGON National Dialogue on Achieving Universal Health Coverage (UHC) in Nigeria provided local government chairmen with a four-step plan:
- Allocate newly autonomous statutory funds to upgrade primary health centres so they meet accreditation standards.
- Collaborate with State Health Insurance Agencies to enrol informal sector workers using flexible micro-premium structures.
- Personally lead public awareness campaigns, involving traditional and religious leaders, to dismantle cultural and low trust in prepayment and fear of extra costs.
- Allocate dedicated budget lines for insurance subsidies to reduce diversion, delay and discretionary spending.
In a separate session on digitising front-line health data, participants called on local governments to consistently capture facility reporting, support connectivity and reliable power at the ward level, and ensure health workers use digital tools rather than leave them idle.
A broader communiqué led by the National Primary Health Care Development Agency (NPHCDA) went further, calling on states and local governments to pool BHCPF, donor and philanthropic funds into a single basket fund with dedicated, auditable accounts at every level.
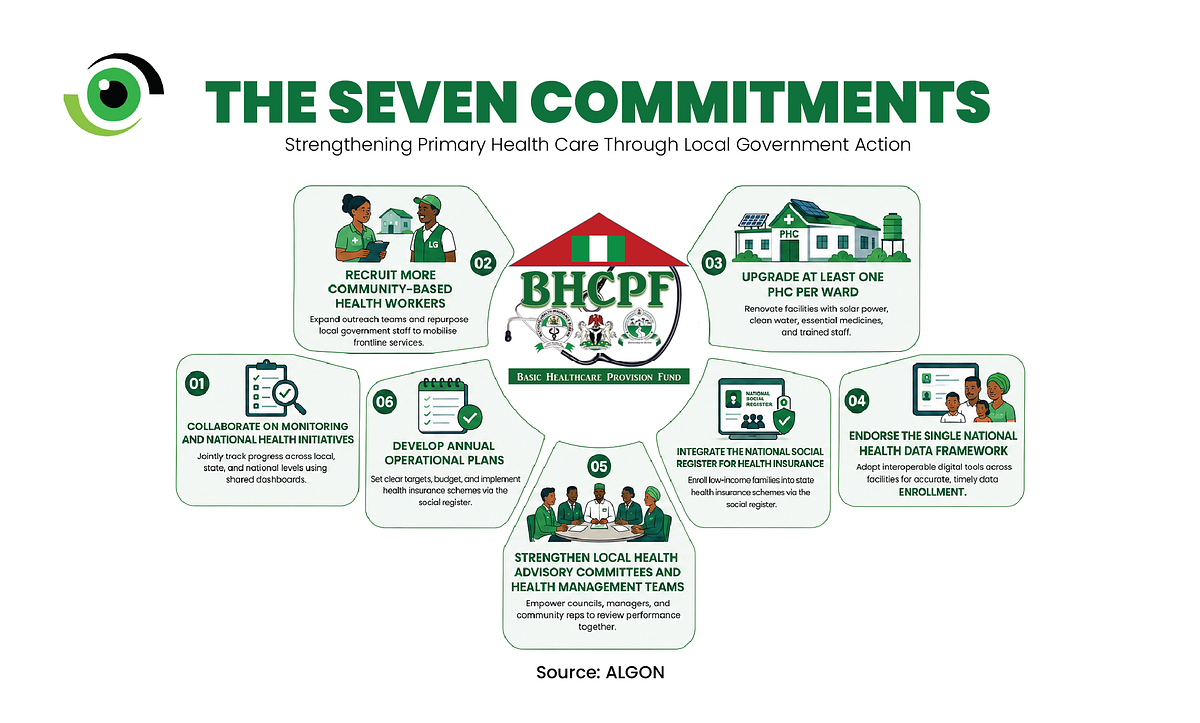
ALGON’s chairmen answered with seven written commitments of their own. Each commitment answers a gap the MAMII data had already made hard to ignore.
Capacity, not a new job description
Representing the Chairman of ALGON at the dialogue, Dr Ben Nkechika, ALGON Health Desk Technical Lead/National Coordinator, rejected the suggestion that local government autonomy had created new responsibilities for councils. Speaking to Nigeria Health Watch, he argued that the responsibilities had always existed, but local governments had lacked the capacity to fulfil them.
“The local government don’t have increased responsibility…The responsibility has always been there. They have not just been capacitated to deliver on those responsibilities,” he said.
Nigeria’s legal and policy architecture has long placed local government areas (LGAs) within the primary healthcare (PHC) delivery chain, while the Supreme Court ruling has sharpened the question of fiscal accountability. Councils can no longer argue that someone else is holding their funds as an explanation for why services have not improved.
Why this matters more than the headlines suggest
Ultimately, this is no longer just about court judgments or financing formulas, important though both are. It is about whether the local government office closest to most Nigerians, the one that runs the clinic, pays the midwife and keeps essential medicines in stock, can manage public funds, implement reforms and deliver quality care without leaning on higher levels of government to do the job.
Increasingly, Nigeria’s progress on primary healthcare will be determined there, across 774 councils with very different capacities, rather than by any single policy signed in Abuja.
Local government autonomy was never going to save lives on its own, any more than the previous system could. Its success will no longer be measured by federal policy alone, but by whether Nigerians experience better care at their nearest primary healthcare centre.
Leave a Comment
Your email address will not be published. Required fields are marked *
Related Stories




