
COVID-19 Funding Built New Health Infrastructure. Will Nigeria Build on It or Lose It?
Related Stories






Oluwafolakemi Ajala (Guest writer)
The arrival of COVID-19 in Nigeria in early 2020 exposed long-standing weaknesses in oxygen supply, diagnostics, surveillance, emergency response coordination and public health funding. In health facilities, access to medical oxygen was often inadequate and unreliable, and laboratory infrastructure was fragmented. Surveillance systems were under-resourced, and genomic sequencing capacity was limited, unevenly distributed, and not yet integrated at the national scale. These issues were not new, the pandemic simply made them impossible to ignore.
On 25 June 2026, stakeholders gathered in Abuja, to formally close out the COVID-19 Response Mechanism (C19RM) grant, a Global Fund investment implemented through national and subnational structures led by the National Agency for the Control of AIDS (NACA), National Tuberculosis and Leprosy Control Programme (NTBLCP), and Lagos State Ministry of Health(LSMoH) as principal recipients, with implementation roles across different sub recipients.
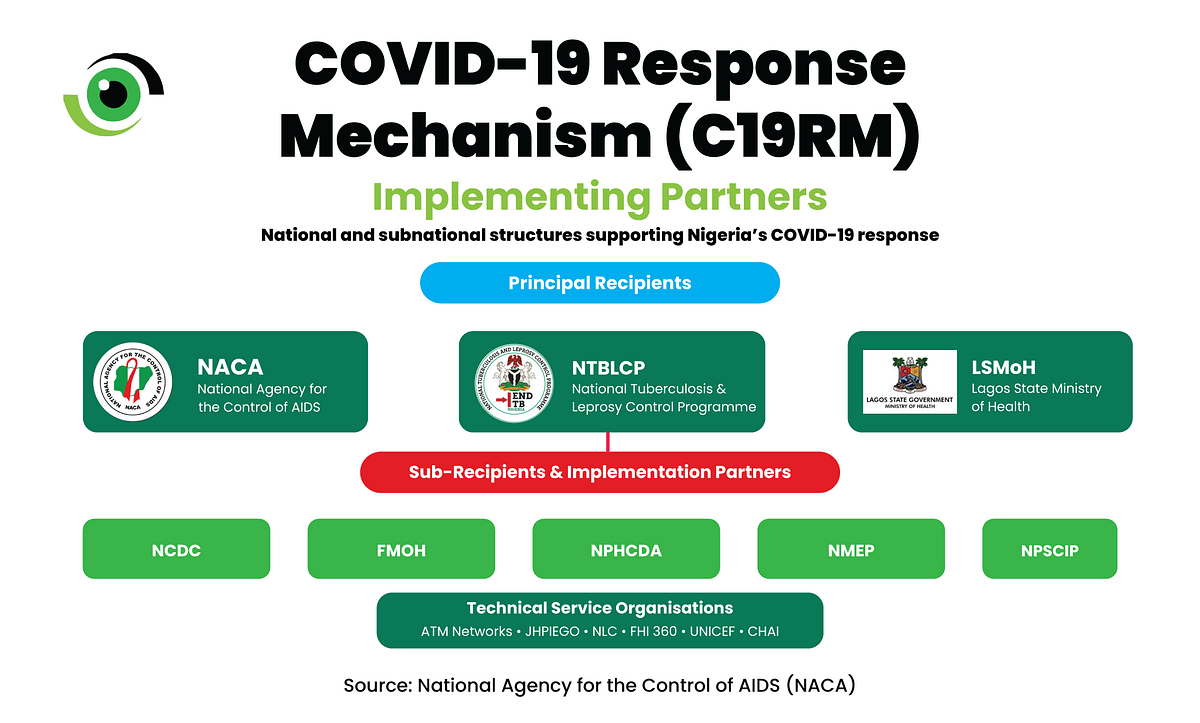
The C19RM was not designed as a narrow COVID-19 response. Rather, the Global Fund structured C19RM to protect HIV, tuberculosis, and malaria programmes from disruption while strengthening the health system capacities on which those programmes depend, including oxygen supply chains, laboratory networks, disease surveillance, genomic sequencing, data systems, warehousing and community health structures.
From assets to ownership
Dr Temitope Ilori, Director General of NACA, set the tone for the meeting in her opening remarks, “Beyond the infrastructure and systems that were established, one of the most important achievements of C19RM has been the partnership that brought together government institutions, development partners, implementing partners, health workers, and communities across the federation. This has helped to strengthen our health systems.”
For Dr Ilori, the most important factor after formally closing out the grant is the sustainability of the investment. The partnerships forged under C19RM are not a by product of the grant; they are the mechanism that made implementation possible at scale and remain the foundation on which sustainability depends.

The true value of the investment will be measured by whether the systems built under C19RM are integrated into routine structures and maintained in the years ahead. This requires accountability at every level of government: federal, state and local.Which ministry, hospital board, or agency is responsible for the maintenance budget for handed-over assets, and are those assets captured in annual operational plans? It is vital to answer these questions because, regardless of their quality at handover, assets degrade without clear institutional ownership.
What the investment changed
The summary presentation by Dr Rhoda Atteh, Project Director of the C19RM Project and Dr Emperor Ubochioma, NTBLCP’s Grant Programme Management Team Lead, detailed a national footprint spanning all 36 states and the FCT.
- 73 new Pressure Swing Adsorption (PSA) oxygen plants were produced and deployed across the six geopolitical zones of the country.

- 12 cryogenic oxygen storage tanks were deployed across the six geopolitical zones.
- 44 tertiary facilities received piped oxygen from source to bedside.
- More than 21,000 oxygen cylinders were procured.
- A national, multi-disease diagnostic and genomic network was strengthened.
- 22 pharmaceutical-grade warehouses were built or upgraded and handed over to the government across twenty-one states.
Beyond infrastructure, the grant strengthened disease surveillance systems by training more than 40,000 surveillance officers to identify, verify, and report diseases of public health importance across event-based, community-based, and routine integrated disease surveillance and response (IDSR) channels.
Dr Ibrahim Tajudeen, Executive Secretary of the Global Fund Country Coordinating Mechanism (CCM), identified the most persistent barrier as the focus on activity-based investment rather than systems investment. “We need to move away from activities-based investment to system investment,” he said, adding that the Principal Recipient-Sub-recipient model required reform.

Lagos State offers an example of how this reform can be successful, as they have been a direct Global Fund principal recipientsince 2017, the only subnational government to hold that position in Nigeria.
Community trust as outbreak infrastructure
Dr Fatima Saleh, Director of Surveillance and Epidemiology at the Nigeria Centre for Disease Control and Prevention (NCDC), emphasised that building community trust is key to combating epidemics. “Not every outbreak is announced through routine reporting channels. Usually, you pick these things through event-based platforms, media reportage, social media and the likes,” she said. Trust is the foundation of outbreak intelligence.
Event-based surveillance, community-based surveillance, and media monitoring are how weak signals become early warnings. They are how a rumour of illness in a market becomes a verified alert in a public health system. Communities share those signals with systems they recognise as theirs. The C19RM investment worked because communities were brought on board, and sustaining the gains requires maintaining this relationship.
Dr Vivian Okafor, who represented the Coordinating Minister of Health and Social Welfare, Prof Muhammad Ali Pate, made it clear that the work ahead is institutional. “The sustainability challenge before us is not merely technical; it requires ownership by governments at all levels, commitment from implementing agencies, continued engagement with communities, and alignment of partner investments behind national priorities.”

The C19RM grant accelerated a national shift toward stronger, faster, and more connected health systems. But acceleration means nothing without maintenance. Oxygen plants fail when the power supply is erratic, there is no preventive maintenance schedule, biomedical engineering support is lacking, oxygen purity monitoring is not in place, or there is no budget to cover any of it.
The same vulnerability applies to pharmaceutical-grade warehouses, GeneXpert platforms, laboratory equipment, and surveillance infrastructure. Lifecycle funding, the recurrent budget that keeps procured assets functional, is critical to sustainability.
What happens when donor funding ends?
C19RM was always designed to move from acute COVID-19 response toward systems strengthening and pandemic preparedness, and that transition now falls entirely to Nigerian institutions. For policymakers, implementers, and decision-makers at every level, domesticising these gains through federal and state budgets, implementation plans, and accountability frameworks is how the grant’s gains will be sustained.
The next phase should consolidate what works and strengthen the response system. Success will be measured by whether these systems still function when the next outbreak comes. Dr Vivian Okafor put it so aptly, “As we close, our focus must shift from emergency response to sustainability.”
Leave a Comment
Your email address will not be published. Required fields are marked *