
Nigeria Cannot Prevent the Next Outbreak if It Cannot Diagnose It

Shalom David and Vivianne Ihekweazu (Lead writers)
In late 2013, Ebola began spreading in Guinea, but the outbreak went undetected for more than three months. Patients arriving at the health facilities presented with fever, vomiting and diarrhoea, symptoms that closely resembled malaria, typhoid, or cholera. Without the diagnostic tools needed to identify the virus, clinicians were unable to determine the true cause of the illness.
By the time Ebola was confirmed, the virus had already crossed into Liberia and Sierra Leone. The outbreak would go on to become the largest Ebola epidemic ever recorded, claiming more than 11,000 lives. Subsequent analysis showed that earlier diagnosis could have reduced transmission. If 60% of patients had been diagnosed within 1 day of symptom onset, rather than 5 days, transmission could have been much lower, highlighting how timely access to diagnostics can alter the trajectory of an outbreak.
This is the scenario currently playing out in the Democratic Republic of Congo (DRC) and Uganda, as in many outbreaks, the window for containment is measured in days. The ongoing Ebola disease caused by the Bundibugyo virus in both countries, which has claimed more than 13o lives in less than two months, initially spread undetected after cases began appearing in mid-April.
One contributing factor was that GeneXpert, a widely used diagnostic platform during outbreaks, could not detect the Bundibugyo strain, revealing the persistent need for diagnostics that can rapidly identify emerging and evolving pathogens.
The investment gap in diagnostics
During the COVID-19 pandemic, governments and donors moved swiftly to fund vaccine development and scale up manufacturing. The United States invested billions of dollars through Operation Warp Speed, while COVAX delivered nearly two billion vaccine doses to 146 economies before closing in 2023. Diagnostics, however, did not attract the same level of political attention or sustained investment.
The Access to COVID-19 Tools Accelerator (ACT-Accelerator) set out to deliver 500 million diagnostic tests to low- and middle-income countries by mid-2021. By the end of that year, only 97 million had been. That gap was significant because outbreaks are controlled through information as much as intervention. Health authorities need to know who is infected, where transmission is occurring, and how quickly it is spreading before they can begin an effective response.
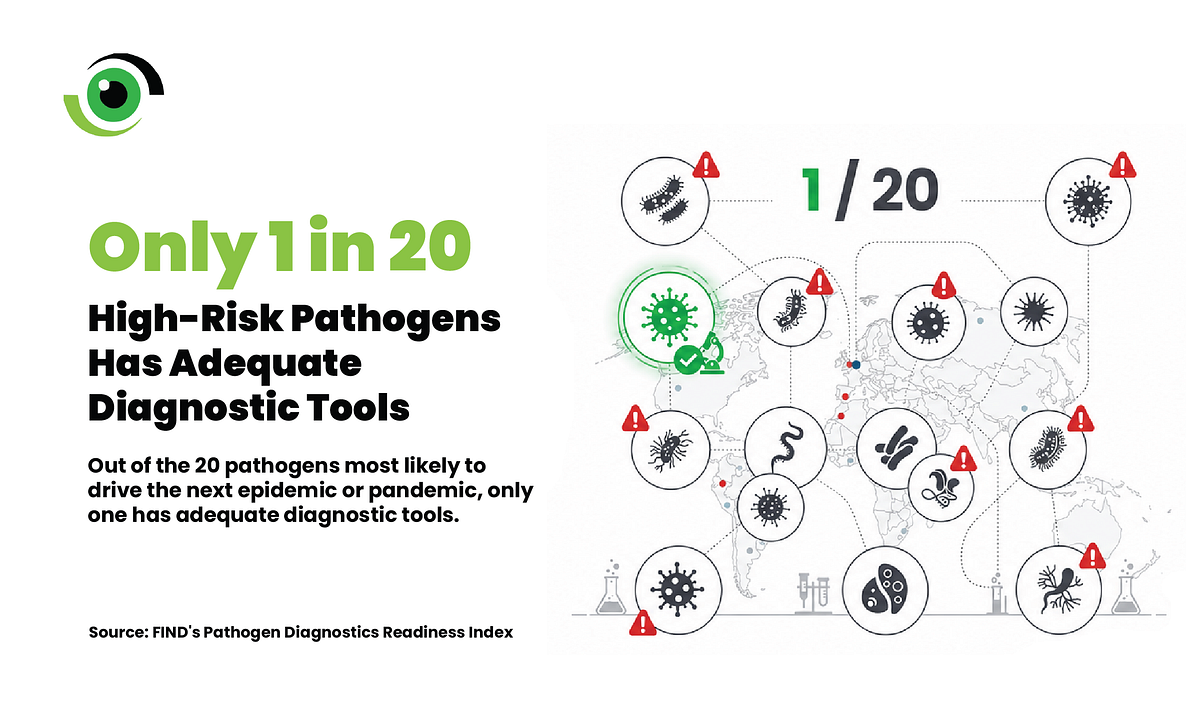
The contrast with vaccines is quite striking. Vaccine development has been enabled by coordinated investments and global partnerships, building a stronger vaccine ecosystem. Organisations such as the Coalition for Epidemic Preparedness Innovations (CEPI) support research and development and efforts to improve equitable access to vaccines, while Gavi, the Vaccine Alliance, helps ensure vaccines reach the populations that need them through delivery and access financing. However, in the diagnostics space, FIND, the global alliance for diagnostics, works to expand access to quality testing and strengthen diagnostic systems.
Yet diagnostics are often the first tool available when a new outbreak emerges. They determine whether a pathogen is identified early enough to interrupt transmission or whether valuable time is lost while cases multiply. However, significant weaknesses across the diagnostics ecosystem continue to hinder the rapid detection of emerging threats.
For countries such as Nigeria, the question is whether health systems can recognise an emerging threat quickly enough. If the next patient arrives at a health facility with fever, headache, and weakness, how rapidly can the cause be identified, and are health workers equipped to maintain a high index of suspicion when patients do not respond to routine treatment?
Nigeria’s diagnostic gap is already visible
Nigeria’s diagnostic gap is already visible in routine healthcare, with patients receiving incorrect diagnoses, clinicians making treatment decisions without reliable test results, and families spending scarce resources moving between facilities because the first could not provide the necessary testing.
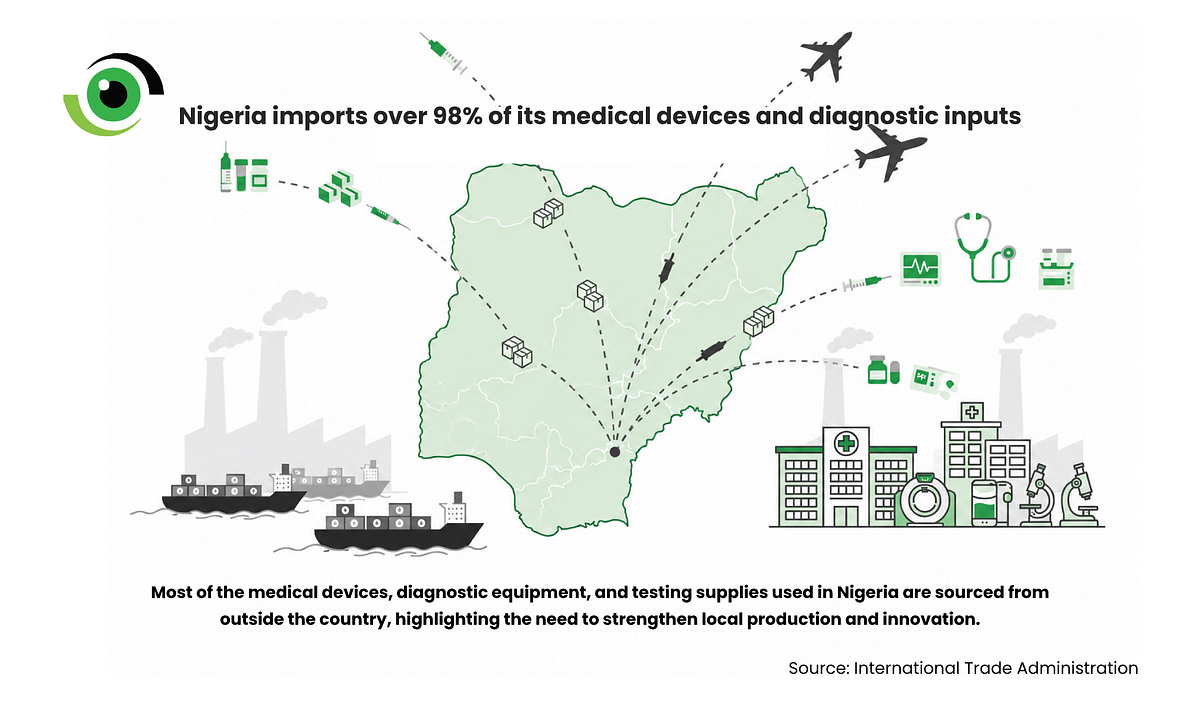
Nigeria remains heavily dependent on imported diagnostic equipment, medical devices, and laboratory inputs, leaving the country vulnerable to foreign exchange fluctuations, supply chain disruptions, delayed procurement, and rising costs. When the next public health emergency occurs, Nigeria could once again find itself waiting for supplies that other countries have already secured. Lassa fever provides a clear example.
Lassa fever shows the cost of late diagnosis
Lassa fever claims hundreds of lives in Nigeria every year. By epidemiological week 21 of 2026, the country had recorded 829 confirmed cases and 208 deaths, with Ondo, Bauchi, Taraba, Edo, and Benue accounting for the majority of cases.
Early symptoms of Lassa fever often resemble malaria and other febrile illnesses. Patients may present with fever, weakness, headache or general discomfort before more severe symptoms appear. Without a rapid, reliable and widely available point-of-care testing, clinicians are forced to make critical decisions with incomplete information.
At Irrua Specialist Teaching Hospital (ISTH), a recognised Lassa fever referral centre, the challenge is immediate. “The cost of test kits has increased significantly in recent years,” said a nurse at ISTH. “We tell patients honestly when we are out of stock and advise them on next steps.”Restoring supplies through the Nigeria Centre for Disease Control and Prevention (NCDC), the World Health Organization (WHO), and partner institutions does not always happen quickly. “Some are resolved immediately,” the nurse said. “Some take much longer.”
For clinicians, the consequences are clinical, operational and emotional. “Surveillance without diagnostics is gossip. Response without diagnostics is guesswork,” said Dr Airefetalor Amanda Ivie, a physician at ISTH. The absence of rapid testing at the frontline also shapes how hospitals respond. If clinicians isolate every patient with a fever, wards can quickly become overcrowded. If they delay isolation, healthcare workers and other patients may be exposed.
“You’re forced to treat empirically,” said Dr Ivie. “For Lassa fever, that means either over-isolating everyone with a fever, causing ward chaos, or under-isolating and risking exposure. Clinicians end up in a ‘damned if you do, damned if you don’t’ situation. Most times, we start ribavirin, and the result comes back negative.”
The costs extend beyond clinical care. Delayed diagnosis affects patient outcomes, healthcare worker safety, health system efficiency and public trust. When families travel long distances, pay out of pocket and still lose loved ones before a diagnosis is confirmed, confidence in the health system can erode.
“It feeds the ‘hospital can’t help’ narrative,”said Dr Ivie. “And that makes community surveillance harder next outbreak.” For Dr Ivie, the challenge is not simply the absence of a test. “The gap isn’t usually ‘we don’t have a test.’ It’s ‘we don’t have the right test, at the right time, at the right place, with results we can act on.’ That’s what turns preparedness plans into stress on the ward.”
Capacity at the top, weakness at the base
The NCDC has strengthened national reference laboratory systems and laboratory networks for priority diseases. Genomic surveillance capacity has expanded beyond COVID-19, while the Institute of Genomics and Global Health has contributed to outbreak detection, sequencing, workforce development and open data sharing.
These investments are important. However, strong reference laboratories are not enough if primary health centres, general hospitals and frontline clinicians cannot access the right test at the right time.
Nigeria needs a diagnostic system that can reliably connect patients in health facilities to laboratories. Tests must be available at the point of care, samples must move efficiently through the health system, and results must be reported promptly. Without these foundations in place, even the best laboratory capacity will struggle to deliver the timely diagnoses needed for outbreak detection.
From policy ambition to implementation
Nigeria’s policy direction is beginning to recognise the importance of local production. The Presidential Initiative for Unlocking the Healthcare Value Chain (PVAC) was established in 2023 to strengthen the local manufacturing of health products and technologies. This ambition was reflected in the 2nd National Diagnostics Summit in March 2026, themed “Strengthening Partnerships and Local Content for Integrated Diagnostics.”
The summit highlighted critical challenges, including workforce shortages, fragmented financing, and a market often shaped more by commercial incentives than by Nigeria’s disease burden. However, Nigeria still needs diagnostics-specific financing, research and development and production capabilities.
Build before the next outbreak
In 2025, the WHO and the Medicines Patent Pool licensed Codix Bio to produce rapid diagnostic tests using SD Biosensor technology, initially for HIV but adaptable for malaria, syphilis, and future health emergencies. Codix Bio has now established a large-scale diagnostic kit plant in Ogun State, capable of producing over 147 million test kits annually.
But the local assembly is not fully independent. “Even when final assembly takes place within Nigeria, we depend almost entirely on foreign inputs for reagents, enzymes, antibodies, plastics, etc.,” Mr Ogunjimi said.“Until we develop this local capacity, any global disruption will directly lead to a domestic diagnostic crisis.”
That is why Nigeria needs a broader approach to diagnostics than simply building a factory or convening a summit.
1. PVAC should establish diagnostics-specific targets and timelines.
2. The Federal Ministry of Health and Social Welfare (FMoHSW), NCDC, the National Health Insurance Authority (NHIA), and state governments should enter into multi-year procurement agreements for essential diagnostics, with local content targets and clear quality requirements.
3. NHIA should use the Essential Diagnostics List to create genuine demand for priority tests, especially for Lassa fever and neglected diseases.
4. Nigeria should also actively participate in global diagnostic platforms, such as the Global Diagnostics Coalition, while shaping the agenda for diseases that affect Nigeria and the West African region.
The next outbreak will not announce itself; it may arrive quietly at a clinic with a patient presenting with fever, headache, and weakness. Symptoms that are easily mistaken for malaria or any number of other common illnesses.
Whether that patient becomes the first detected case or the start of a wider outbreak will depend on whether the right test is available, whether samples can be transported and processed, the speed and accuracy of diagnosis, and whether results are reported quickly enough to trigger an effective public health response.
Diagnostics are the entry point to care, the foundation of effective surveillance, and a critical component of epidemic preparedness. Whether Nigeria can prevent, detect and respond to the next public health threat will depend on the strength and resilience of its diagnostic ecosystem.
Leave a Comment
Your email address will not be published. Required fields are marked *
Related Stories




