
How a Zambian Community Turned Local Reports into an Early-Warning System
Related Stories






In Kanyama, a peri-urban settlement in Lusaka, Zambia, thirty-five-year-old Emmanuel Banda begins many mornings by moving house to house through the community where he lives and works. Banda is a polyvalent community-based volunteer, a health worker trained across multiple disease areas rather than one, to identify health risks before they escalate into emergencies. Kanyama is divided into 11 units, neighbourhood clusters that organise the settlement into manageable zones for health service delivery. During a routine visit to Unit 1, Kanyama Site and Service, one household caught his attention.
Three people in the community had been experiencing watery diarrhoea for three days. They had tried medication, but the symptoms had not stopped. A child next door had similar symptoms. Emmanuel remembered his training, brought out a small notebook, and wrote down a code. The notebook is called the Rumour Logbook.
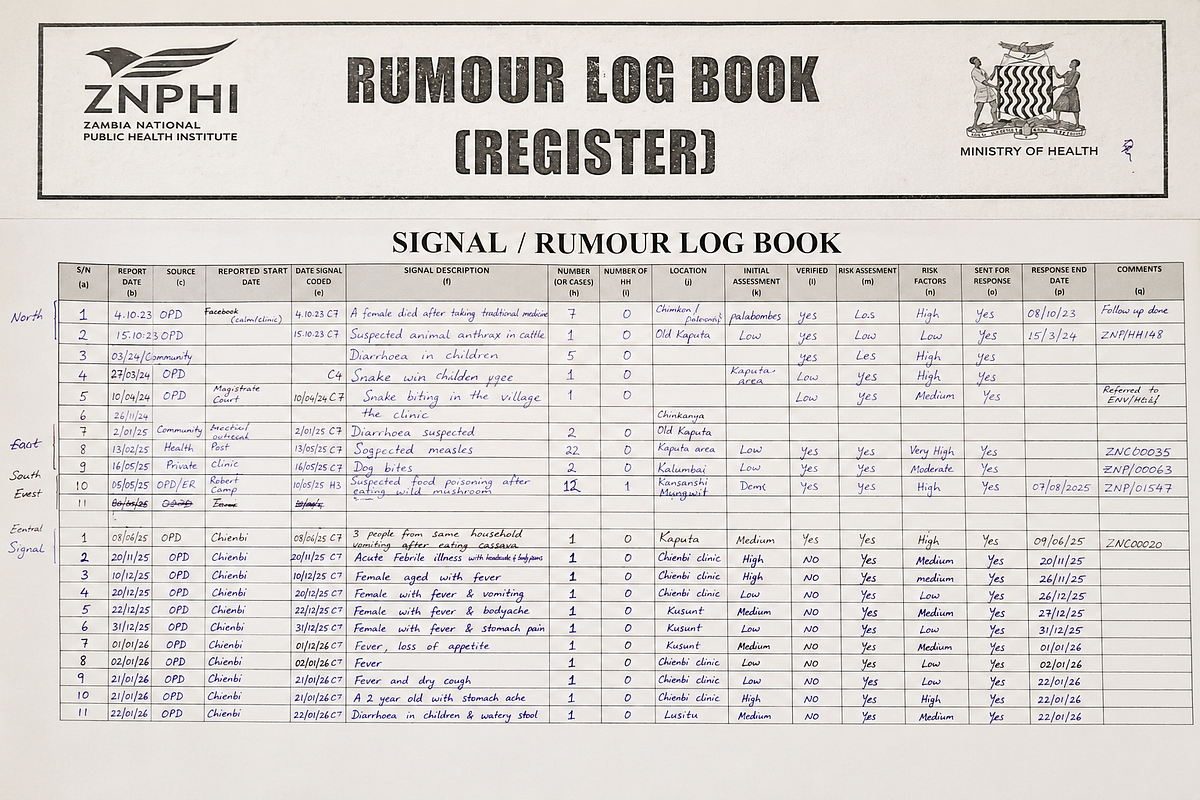
Image credit: Nigeria Health Watch
A notebook that carries early warnings
The Rumour Logbook is part of Kanyama’s community event-based surveillance system. A “rumour” here is not dismissed as gossip, it is an unverified report of an unusual health event that may require investigation. The Zambia National Public Health Institute (ZNPHI) describes event-based surveillance as the detection and reporting of unusual or unexpected health events, including outbreaks and case clusters.
In Kanyama, community-based volunteers (CBVs) use the logbook to record unusual events. A cluster of diarrhoea cases in one household, flooding that could contaminate a water source, or suspected food poisoning. Each event type has a code that helps volunteers log it, and the facility decides which rumour needs urgent attention.
“When a volunteer fills in their small book, they are not just recording a complaint,” explains Enala Mbao, the community focal person for Kanyama. “They are also providing a landmark, the location of the affected household, the contact details of the family, the number of people involved, everything a surveillance officer needs to decide whether what has been reported is a signal worth investigating or a confirmed event requiring an immediate response.”

Every Friday, the books are returned to the facility, where the surveillance officer maintains a master logbook consolidating reports across Kanyama. But urgent cases do not wait. “When there is an emergency, we won’t wait until we bring the book back,”Emmanuel says. “We call the facility the same day we find the cases.”
Following the Rumour
When Emmanuel arrived at Elizabeth’s home, the setting was familiar. Open drains and poor sanitation were visible reminders of why outbreaks of waterborne diseases such as cholera occur so easily in communities like this. Elizabeth had been caring for three sick relatives. She had bought tablets from a nearby drug shop, hoping the symptoms would subside.
But no one had gone to the health facility because missing even a single day’s work meant losing income the family depended on. “We all drank the maize drink that day, but I don’t know what made us sick,” Elizabeth said. “Maybe it was the drink, maybe it was the water. We only had enough money to buy food. Buying chlorine to treat our water is not something we can afford.”

Image Credit: Nigeria Health Watch
Emmanuel asked the questions he had been trained to ask. What had they eaten? What were they drinking? Where was the water coming from? The answers suggested possible contamination. “When you look closely, the disease isn’t the real problem,” Mr Banda said. “The real issue is sanitation. We keep seeing the same conditions. Poor toilet facilities, untreated household water, and waste disposed near drainages that floods carry straight back into people’s homes.”
After Emmanuel alerted the health facility, a team accompanied him back to the community to conduct a household investigation. Going from house to house, they searched for additional cases and traced contacts, documented what people had eaten and drunk, collected water and maize-drink samples, distributed chlorine, and sensitised neighbouring households on how to prevent further spread.
Elizabeth said she was relieved he had come because health workers rarely reached that part of the community. “They come around the community,” she said. “Seeing them around really helps us feel closer to the health facility.”
Kanyama’s long history of cholera
Kanyama has long been one of Lusaka’s cholera hotspots. A 2024 study found that Kanyama sub-district was the origin of major Lusaka outbreaks in 2005–2006, 2016 and 2017–2018, and that a lack of sanitary toilet facilities was associated with increased cholera cases.

In October 2023, ZNPHI reported a cholera alert from Kanyama and listed operational gaps there, including erratic water supply, inadequate support for volunteers, accumulated solid waste, and reliance on untreated shallow wells and boreholes.
The outbreak became one of Zambia’s worst. Between 15 October 2023 and 23 July 2024, Zambia recorded 23,382 cumulative cholera cases and 740 deaths, with Lusaka the epicentre and, in January 2024, accounting for 75% of all cases nationwide.
The people who carry the system
Kanyama’s health network runs on two types of volunteers. Monovalent community-based volunteers are trained in a single programme area, such as tuberculosis, HIV, or malaria; polyvalent community-based volunteers, like Emmanuel, are trained across many, including environmental health, water and sanitation, and community surveillance. Zambia is rolling out remunerated polyvalent volunteers.

Kanyama currently has 258 polyvalent CBVs, trained with support from partners including Africa Centres for Disease Control and Prevention and UNICEF, and receiving a monthly stipend of 1,300 Zambian kwacha through Global Fund-supported programming under grants worth US$362 million for 2024–2026.
Volunteers are recruited from the zones they serve, selected through neighbourhood health committees for local representation. “These CBVs are chosen from the areas where they are coming from,” says Mbao. “Even as they are doing their service delivery in the community, they do it from where they are coming from.”That proximity is the system’s strength. Volunteers know which households share a water source and which families delay care because of cost.
“Before I became a CBV, I didn’t have the money to start a business or the connections to get a job,” Emmanuel says. “A friend introduced me to the programme and told me all you needed was commitment, a kind heart, and to be from Kanyama. I joined because I didn’t have many options, but today I’m glad I did. I enjoy the work, I enjoy helping people, and I can honestly say becoming a CBV has been worth it.”

Image Credit: Emmanuel Banda/PCBV
What the system has not yet solved
Surveillance alone cannot solve cholera. Kanyama’s structural vulnerabilities, unsafe water, poor sanitation, flooding, and inadequate waste management require long-term investment in water, sanitation, and hygiene. But early detection still changes what happens next, how quickly a household is reached and whether cases are contained before they spread.
The Rumour Logbook is only as strong as the people carrying it, and there are not enough of them. Kanyama has 50 zones and more than 500,000 residents, but only 258 polyvalent CBVs. “Looking at the number of units that we have compared to the number of CBVs that have been trained, we would like the Global Fund to train more CBVs as polyvalent,”Mbao says. “If we can have more CBVs trained, I think we will not have cases of cholera.”
More trained volunteers could improve coverage, early detection and referral. However, volunteers alone will not eliminate cholera, it also requires safe water and sanitation, targeted vaccination, rapid treatment and a responsive health system.
Time is another constraint. “Our time was cut from four to six hours to two hours because it’s not paid, so you can do something else with your time,” says Daniel, a CBV in Kanyama. “Only that in two hours, we couldn’t reach a lot of households.”

Image credit: Nigeria Health Watch
Then there is the paperwork. Every case logged generates a report submitted to the facility, with the volunteer keeping a copy. “There is a lot of paperwork because we have to submit the reports and also keep a copy for ourselves,” Emmanuel says.
The wider lesson
Community-based surveillance works because many outbreaks begin as something people notice before health systems formally record it, a cluster of diarrhoea cases, or a rumour about unsafe water.
Kanyama’s Rumour Logbook uses local volunteers, a small coded notebook, a phone call, a surveillance officer, and a facility expected to respond. It needs no electricity, a smartphone, or internet, but it does require training, supervision, transport, testing supplies, and a health system that takes community reports seriously.
For countries building community health infrastructure beyond donor-dependent, disease-specific programming, Kanyama offers a practical lesson. The most reliable early-warning system in any community is often the people who live there.
Give them clear signals to watch for, a trusted way to report, and a health system that responds, and the notebook in their pocket becomes an early warning tool that helps stop outbreaks before they spread.
Leave a Comment
Your email address will not be published. Required fields are marked *