
The Anatomy of an Outbreak in a Conflict Setting & Nigeria’s Preparedness for Ebola
Related Stories






The latest Ebola outbreak in DRC is unfolding in a conflict-affected region where insecurity, displacement, and fragile trust are complicating containment efforts. What does this reveal about Nigeria’s preparedness for outbreaks in its own most challenging settings?
When the World Health Organization (WHO) declared the Ebola outbreak in the Democratic Republic of Congo and Uganda a Public Health Emergency of International Concern, it was issuing the highest level of alarm available under the International Health Regulations for the ninth time in history, the third involving Ebola, and the first for an outbreak caused by the Bundibugyo strain, for which no licensed vaccine exists.
The declaration reflected growing concern about an outbreak unfolding in a conflict-affected region where insecurity, displacement, and fragile community trust are making containment significantly harder. As WHO Director-General Dr Tedros Adhanom Ghebreyesus stated at the recent media briefing on the Ebola outbreak: “The key to ending this outbreak is not biomedical. It’s leadership, ownership, partnership and trust.”
Nigeria responded with familiar and necessary measures, activating an Emergency Operations Centre (EOC), designating laboratories, and completing a risk assessment, placing national preparedness at 59%. These essential steps are a standard minimum response that most countries with functional public health systems would be expected to mount, but they answer the easier question.
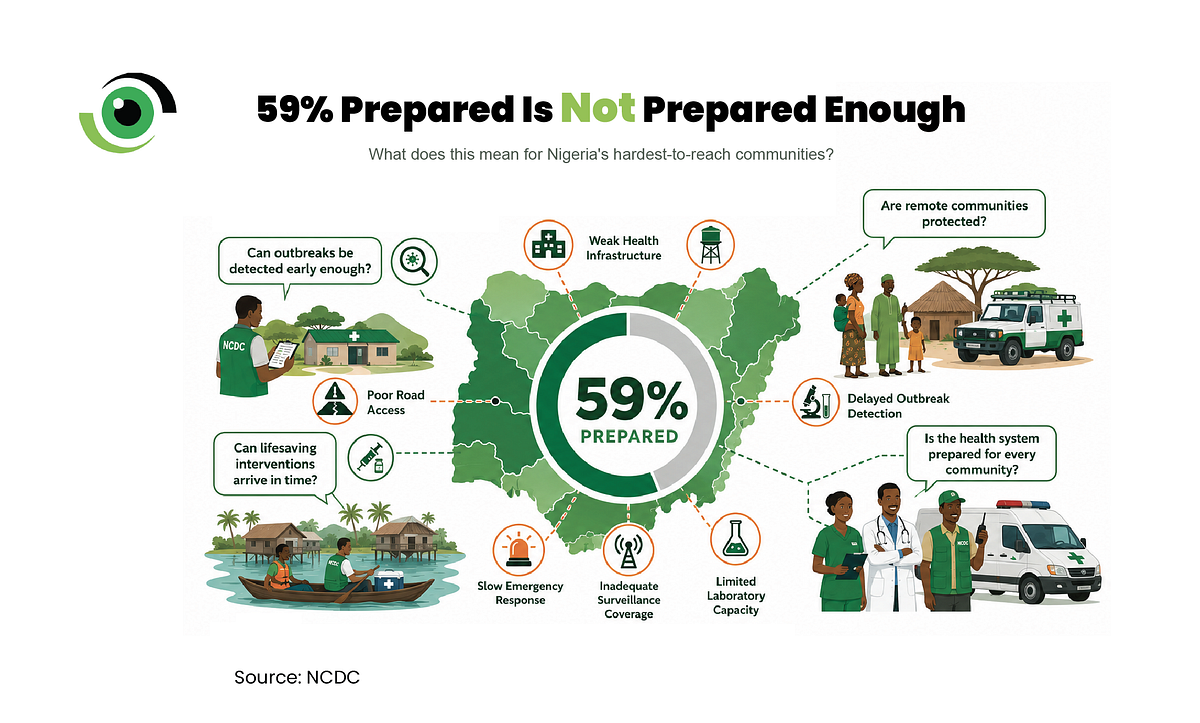
The harder question is what happens if Nigeria’s potential index case does not arrive at an international airport, as in 2014, but instead appears in one of the country’s conflict-affected communities, where years of insecurity have weakened healthcare infrastructure and institutional trust?
Nigeria is not starting from zero
Nigeria’s track record of responding to concurrent outbreaks justifies its preparedness measures. A swift response contained the 2014 Ebola outbreak within weeks through rapid contact tracing, a unified command, and political leadership, lessons that shaped how Nigeria approached subsequent outbreaks.
Years of Lassa fever surveillance coordinated through NCDC’s National Reference Laboratory strengthened diagnostic systems that would prove critical during COVID-19, when the NCDC built directly on that foundation to achieve a record expansion of testing laboratories, train more than 35,500 health workers on infection prevention, and develop genomic sequencing capacity now extended across multiple pathogens.
More recently, investments in clinical trial readiness for Lassa fever across high-burden states are beginning to build the institutional research infrastructure that could underpin epidemic preparedness. At a recent emergency meeting convened by the House of RepresentativesCommittee on Healthcare Services, which Nigeria Health Watch attended, NCDC Director General Dr Jide Idris updated the House on Nigeria’s preparedness for Ebola.

In a subsequent Arise TV interview, he was direct: “I’ll be frank with you, we are not 100% ready, but we are improving our readiness. With a new Ebola outbreak now declared, a critical question is how much of the infrastructure built during the 2014 Ebola response and the COVID-19 pandemic has been sustained well enough to mount a robust response today.
The realities shaping Nigeria’s outbreak readiness
An outbreak risk assessment evaluates multiple pillars of preparedness, from the likelihood of importation and spread, to capacity for prompt diagnosis, surveillance at points of entry, and health workforce readiness. The outbreak in the DRC shows that preparedness depends on how those pillars perform under conditions of insecurity, population displacement and weak institutional trust.
Nigeria faces multiple security challenges across different parts of the country. Fifteen years into the northeast crisis, approximately 2.3 million people have been internally displaced across Borno, Adamawa, and Yobe, with 5.9 million requiring humanitarian assistance and 31% of health facilities out of operation during recent crisis periods. Beyond the northeast insurgency, Nigeria has been ranked the fifth most dangerous country globally in December 2024, with around 15,000 kidnappings recorded between 2019 and 2025. These same conditions of insecurity and displacement are also making it harder to contain the outbreak in eastern DRC, where the WHO says contact tracing coverage must increase from 45% to more 90% to bring transmission under control.
The trust deficit runs deeper still. During the COVID-19 outbreak, research found that 56.8% of Nigerians surveyed mistrusted the government, and this mistrust was directly associated with lower vaccine acceptance, a pattern confirmed across multiple studies. In the event of a potential Ebola response, where isolation and contact tracing are the primary containment tools, that trust deficit could make it harder to control the outbreak.
Preparedness is built long before the crisis
As Dr Chikwe Ihekweazu, Executive Director of the WHO Health Emergencies Programme, observed, “To build trust in the people you serve, you have to be there for them all the time. Whether it’s a woman giving birth, a child brought for immunisation, or treatment for malaria, if you’re not able to solve their day-to-day problems, why do you expect them to welcome you when there’s an Ebola outbreak?”
Dr Abdi Mahamud, WHO Director for Health Emergency Alert and Response Operations, drew a similar connection when he said: “What is critically different is starting with the community, but going all the way up to heads of state and ministries of health.”
For Nigerian policymakers and health authorities, this points to important gaps that preparedness assessments can miss, including whether trusted voices are available to support effective risk communication, whether health services can continue to function in insecure settings, and whether cases can be rapidly detected and investigated in areas with the weakest state presence.
For health workers, early detection and infection prevention are key, but preparedness cannot rest on their shoulders alone, particularly in environments where their own safety cannot be guaranteed. For ordinary Nigerians, the right response is awareness, seeking information from trusted sources and avoiding the spread of misinformation, not alarm. This means understanding how Ebola spreads, seeking care early if symptoms develop, and following guidance from Nigeria’s national public health institute, the Nigeria Centre for Disease Control and Prevention (NCDC).
Nigeria has demonstrated the capacity to respond to public health emergencies. However, preparedness is not a permanent achievement, but the result of a sustained investment in a coordinated public health architecture and strong supporting institutions. While the 59% preparedness score provides an important measure of current readiness, the lesson from eastern DRC is a reminder that outbreaks often expose the weakest link in the health system. That is why preparedness must be built long before an emergency and sustained long after the immediate threat has passed, and why its true test comes only when a new threat emerges.
Leave a Comment
Your email address will not be published. Required fields are marked *