
Africa’s Precision Medicine Future Depends on Stronger Research and Clinical Trial Systems
Related Stories






Olatunde Olaoluwa and Prudence Enema (Lead writers)
Precision medicine will not deliver equity for Africa if Africa remains underrepresented in the evidence that shapes it. The endorsement of a new resolution on Precision Medicine at the 79th World Health Assembly reflects an important step towards health equity and Universal Health Coverage. This decision was endorsed by all member states.
In support of this, the World Health Organization (WHO) is mandated to provide technical and normative guidance, coordinate existing frameworks, facilitate global collaboration, review and map existing WHO guidance and, if necessary, consider developing a global strategy on precision medicine, alongside tools such as a country maturity model to help states assess their readiness and implementation capacity.
Precision Medicine is a healthcare approach that uses detailed information about a person’s genetics, molecular and lifestyle characteristics, as well as clinical data, to better understand, prevent and treat disease. It enables healthcare providers to tailor prevention, diagnosis, and treatment to an individual’s specific characteristics, leading to more accurate diagnoses, more effective treatment, and improved health outcomes.

Population-based medicine remains essential, but standardised approaches can miss important biological and clinical differences between individuals. As a result, some patients experience variations in diagnostic accuracy, treatment response, safety monitoring, and health outcomes.
This approach is limited because it assumes patients will respond similarly to the same interventions, treating populations as statistical averages rather than recognising that individuals differ in their genetic makeup, environmental exposures and biological responses.
Precision medicine offers more targeted prevention strategies, earlier and more accurate diagnosis, and treatments better matched to individual biology and context. However, this promise raises a fundamental question for Africa. ‘Can precision medicine be equitable if the evidence base is not?’
Africa’s disease burden and evidence gap
African populations are home to the greatest human genetic diversity, shaped by complex population histories and a wide range of environmental, social, and cultural conditions. Consequently, health outcomes and responses to treatment in these settings are influenced by multiple, often overlapping factors, including a continuing high burden of infectious diseases, such as Lassa fever, mpox, tuberculosis andmalaria. This is alongside a growing burden of noncommunicable diseases such as hypertension, diabetes, cardiovascular disease and cancer.
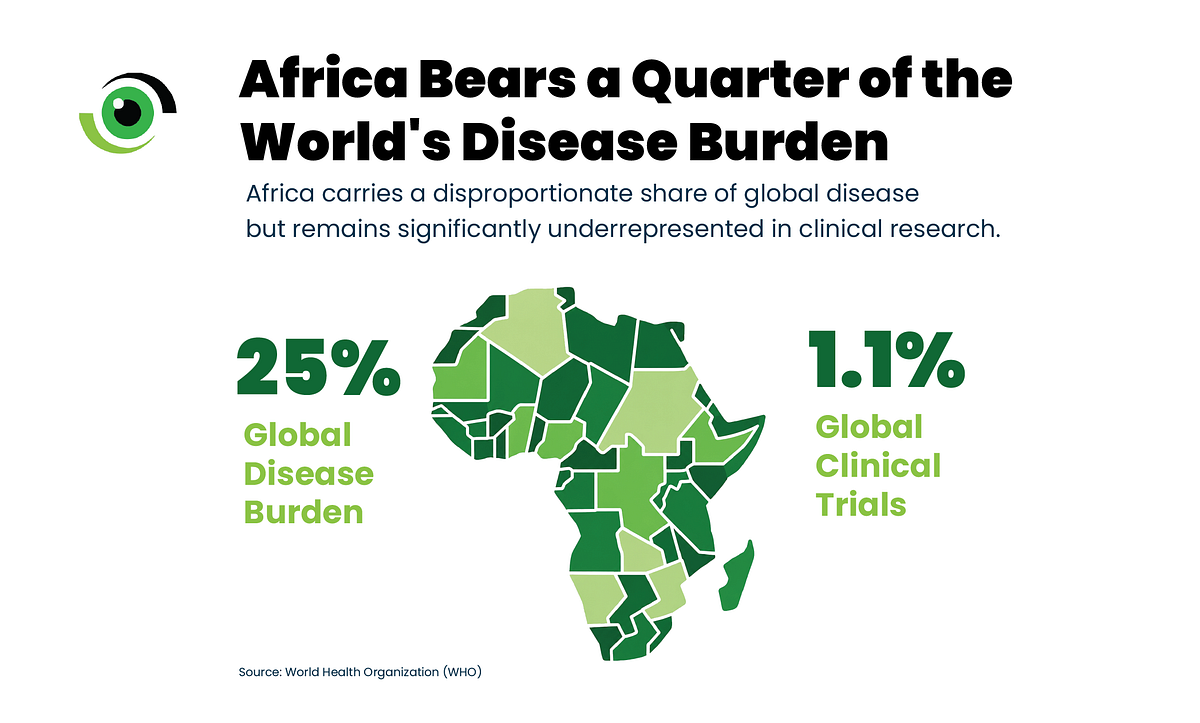
The coexistence of these conditions creates complex clinical profiles that may not be well captured in studies conducted in settings with different ancestry profiles, disease burdens, nutrition patterns, health systems and environmental exposures. Yet, of the over 20,000 trialsinitiated each year globally, fewer than 1,000 are typically hosted in African countries. In contrast, North America, Europe, and Asia combine for over 90% of global interventional trial registrations.
In 2023, of the 20,825 trials that started globally, only 819, about 4% of the total, were hosted by African countries. This underrepresentation is mirrored in genomics, where African populations are poorly represented, accounting for less than 2% of the genetic data analysed in genomics research.
The evidence base that informs global therapeutics is often derived from a relatively narrow segment of global human diversity. This creates bias in the knowledge systems that guide drug development, diagnostic tools and treatment protocols.
Precision medicine relies on large, high-quality datasets to tailor health interventions to specific populations. However, many African countries remain significantly underrepresented in the research platforms, clinical trials, and drug development processes that drive modern healthcare innovation.
In many African settings, co-infections such as HIV and tuberculosis, malaria in pregnancy, malnutrition, and environmental exposures can affect disease progression and treatment response.
Nutritional status, diet, and differences in microbiome–drug interactions (the bidirectional relationship between pharmaceutical drugs and the human microbiome) further influence drug absorption and efficacy.
Environmental exposures, including climate conditions, pollution, and endemic pathogens, add additional layers of complexity to disease progression and treatment outcomes.
In this context, applying evidence generated outside the continent without sufficient local validation risks limiting the effectiveness of even the most advanced medical innovations.
Building the foundation for precision medicine in Africa
The World Health Assembly’s endorsement of precision medicine represents a policy signal, and a strategic inflexion point for regional bodies such as the Africa CDC, the West African Health Organisation (WAHO) and the African Medicines Agency (AMA).
It presents Africa with an opportunity to connect genomic and health data infrastructure, clinical research networks, R&D ecosystems, local manufacturing capacity, and harmonised regulatory frameworks. Together, these pillars can enable the continent to move from being a passive recipient of externally generated innovation to an active participant in shaping the future of global health.
At the same time, the resolution raises an urgent question: ‘Will precision medicine help narrow longstanding health inequities, or will it deepen them by concentrating benefits in countries with stronger scientific and technological ecosystems?’
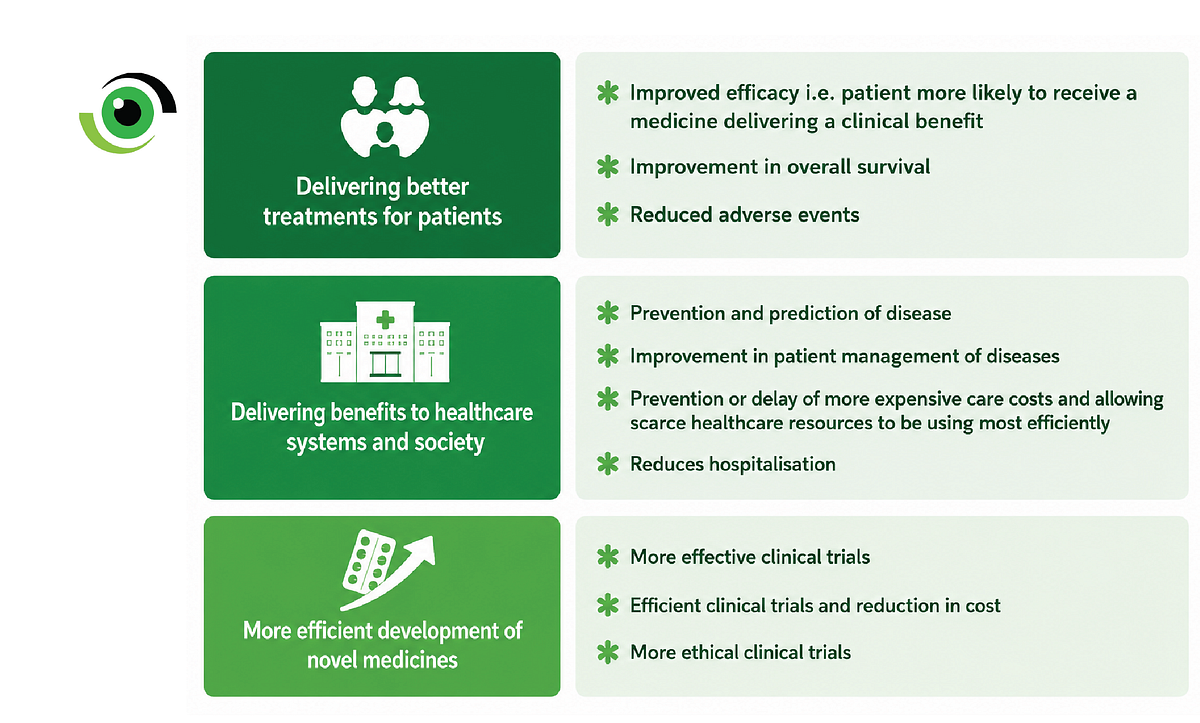
Image credit: Nigeria Health Watch
R&D is the infrastructure of precision medicine
Precision medicine depends on continuous cycles of evidence generation, validation and adaptation. This requires strong research and development (R&D) ecosystems capable of generating the scientific knowledge needed to understand how biological, environmental, and epidemiological differences shape health outcomes across populations.
A report by the Africa Centres for Disease Control and Prevention (Africa CDC) and Team Europe Initiative estimates that every dollar invested in health research and development on the continent could generate up to $137 in economic returns and create approximately 4.56 million jobs by 2044.
Investing in R&D, therefore, serves a dual purpose. It strengthens Africa’s capacity to contribute to and benefit from advanced precision medicine, while also generating substantial economic returns. More importantly, it positions the continent to move beyond reliance on externally developed innovations towards shaping solutions that are scientifically relevant, economically sustainable, and responsive to African health priorities.
For Africa, the answer will depend on whether the continent invests not only in adopting precision medicine tools, but in building the systems required to produce, validate, and adapt them within African contexts. Africa must not only receive precision medicine; it must help define, test, regulate, finance and govern it.

As Dr Sylvie Briand, WHO Chief Scientist, put it:”By uniting people-centred healthcare with innovation, precision medicine has the potential to transform lives. This resolution helps ensure those advances serve the shared goal of health for all.”
Leave a Comment
Your email address will not be published. Required fields are marked *