
First Call, First Care: Why Nigeria Must Protect the Nurses Who Protect Us

Damilola Ilori and Tosin Emejor (Lead writers)
“Go and call Aunty Nurse.” In many Nigerian households, this phrase evokes both fear and relief. It is used when a child’s fever spikes, a pregnant woman senses something is wrong, a wound needs dressing, or an elderly parent has high blood pressure.
For many Nigerians, the first trusted health worker is the nurse at the local clinic. Long before a patient enters a consulting room, a nurse may have already checked vital signs, identified danger signs, or advised urgent care.
Behind this familiar phrase are real lives. A young woman whose wound healed because a nurse noticed a missed step, a woman whose long search for pregnancy care changed because a nurse asked the right question, and an older man who still manages his blood pressure because a nurse became his family’s steady guide.
Against the backdrop of International Nurses Day 2026, under the theme “Our Nurses. Our Future. Empowered Nurses Save Lives,” Nigeria must reflect on whether we are truly empowering nurses or merely relying on them until they become overwhelmed.
The backbone of a stretched system
Nurses are central to primary health care in Nigeria. They educate, counsel, immunise, monitor pregnancy, support childbirth, manage chronic conditions, and respond to emergencies. When nurses receive proper training, payment, protection, and equipment, prevention is brought closer to families and maternal and newborn care is enhanced.
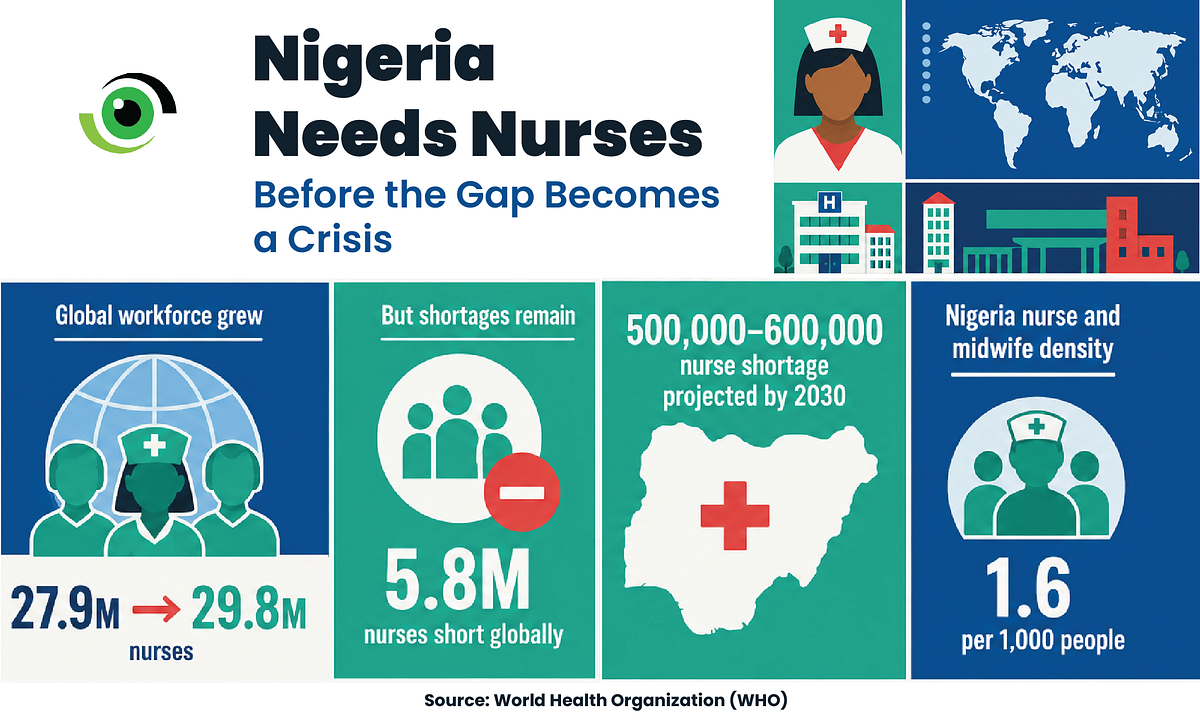
Globally, the nursing workforce increased from 27.9 million in 2018 to 29.8 million in 2023, yet there remains a shortage of 5.8 million nurses. Nigeria’s outlook is concerning. An estimated shortage of 500,000 to 600,000 nurses is projected by 2030 if the country does not expand and retain its nursing workforce.
The Federal Government reports a rise in nursing and midwifery enrolment from 28,000 in May 2023 to 110,000 in 2024/2025. Additionally, over 70,000 frontline health workers have been retrained, and more than 20,000 health workers, mainly nurses and midwives, have been recruited. However, training alone is inadequate; it must be complemented by funded jobs, fair pay, and clear retention pathways.
Nigeria struggles with overcrowded wards, delays in care, exhausted healthcare workers, overstretched primary healthcare centres (PHCs), and families often contacting one nurse because the formal system feels too distant, slow, or expensive. The country’s nurse and midwife density is about 1.6 per 1,000 people.
Women make up 85% of the global nursing workforce, highlighting the gendered nature of care work. However, nursing should not be viewed as a woman’s sacrifice, nor should male nurses be made invisible. The profession includes both women and men whose labour, judgement, skill, and leadership are essential to health systems.
Nigeria reflects this gendered reality. Women make up about 87% of nurses and midwives. This makes nursing not only a workforce issue but also a matter of decent work, gender equality, and the care economy.
When support is missing
Nigeria’s Task-Shifting and Task-Sharing Policy aims to broaden access in areas with staffing shortages. It is effective when supported by training, supervision, supplies, referral systems, fair pay, and legal protection. Without these elements, it risks becoming merely another form of overwork.
In many facilities, nurses do more than share tasks. They also bear the brunt of system failures. They step in for absent doctors, cope with staffing shortages, fix broken referral processes, and manage empty shelves, all while carrying out their own duties.
This unseen work saves lives before the system recognises it. Adaeze avoided a potential wound infection because a nurse neighbour knew her dressing should have been done earlier. Hasanatu conceived after nine years because a nurse asked the missing question about hormonal assessment. Mr Chibuzor still manages his blood pressure because Nurse Abel became his family’s steady guide through diabetes, loss, and ageing.
Migration is a symptom
Nurse Ronke worked at a general hospital for twenty years. After two years in the emergency ward, she asked for a transfer due to chronic understaffing, traumatic cases, and exhausting hours. “I had to request a transfer after two years in the emergency ward. The understaffing, traumatic cases, and exhausting hours took a significant toll on me, physically and emotionally,” Nurse Ronke said.
Her story is not uncommon. Many nurses work long shifts, face unsafe nurse-to-patient ratios, do poorly paid or unpaid overtime, and have limited protection from violence, infection, stress, and exhaustion. The State of the World’s Nursing 2025 report found that only 42% of responding countries had provisions for nurses’ mental health support.
Nigeria does not have specific public data on nurse mental health support, but the warning signs are already clear. Poor working conditions, unsafe staffing, industrial unrest, and migration all point to a workforce under considerable strain.
The current nurse migration should not be blamed on nurses. Instead, it highlights broader systemic issues. In 2025, nurses in Nigerian public hospitals launched a warning strike over pay, working conditions, and recruitment. Meanwhile, the union observed that over 42,000 nurses left Nigeria for international employment between 2022 and 2024.

Appreciation is not enough
Every year, nurses are commended for their sacrifice. However, sacrifice is not a sustainable workforce strategy. Nigeria cannot base its health policy on the assumption that nurses will always bear the burden.
Federal and state governments must recruit and retain more nurses, especially in PHCs, maternity units, emergency departments, neonatal units, rural facilities, and high-volume hospitals. Safe staffing standards should be developed, funded, and enforced where understaffing most directly costs lives.
Nurses need fair pay, paid overtime, rural retention schemes, functional equipment, protective supplies, safe workplaces, mental health support, specialist training, and career pathways that do not penalise them for staying in their roles.
They also require formal participation in health workforce planning, primary health care restructuring, maternal and newborn health policy, quality-of-care committees, and health facility budgeting.
Training more nurses without employing, paying, supervising, and retaining them simply increases the pipeline for migration. Nigeria requires nursing schools, but it also needs funded jobs, decent working conditions, and a health system that values the people it trains.
The proposed Afreximbank–King’s College London Medical and Nursing School in Abuja reflects an investment in health workforce training, but it is still within the African Medical Centre of Excellence (AMCE)’s future expansion phase. For Nigeria, new schools must be supported by funded jobs, safe staffing, fair pay, supervision, and career pathways that enable staff to remain in their roles.
The phrase “Aunty Nurse” may be common, but the lesson it holds is much larger. Nurses, both women and men, have always been the primary caregivers for families and communities. If Nigeria wants them to keep saving lives, it must stop seeing them as endlessly available and start recognising them as essential health workers.
Leave a Comment
Your email address will not be published. Required fields are marked *